
New Trends In Clinic Design

Credit: Michael McLane Photography, Courtesy of Taylor Design.
With consideration for the patient experience upon arrival, the UCSF Heart & Vascular Center, which opened in April and consolidated the system’s cardiovascular services under the roof of a multidisciplinary clinic, is designed so that patients are immediately greeted by a staff member and a panoramic view of San Francisco.

Credit: Steve Henke.
The staff area at HealthEast’s Tamarack clinic borders the back doors of the facility’s exam rooms. Supplies are stocked via the narrow doors adjacent to the exam room entrances.

Credit: Steve Henke.
HealthEast’s Clinic – Tamarack in Woodbury, Minn., designed by HGA and completed in 2015, offers an example of a separate consultation space in the exam room to support patient/physician interaction, away from the exam table.

Credit: Halkin Mason Photography.
The Tisch Center for Men’s Health at New York University Langone Medical Center in New York, designed by Perkins+Will and opened in January 2014, uses a rich materials palette and harvests natural light from exterior windows. “These spaces, in some ways, should be better than the best restaurants you go to. It’s an uplifting experience, so you feel like, hey, this isn’t so bad,” says Ted Shaw, associate principal at Perkins+Will.

Credit: Assassi Productions, Courtesy of Taylor Design.
Dedicated office space in the Scripps Clinic John R. Anderson V Medical Pavilion in La Jolla, Calif., designed by Taylor Design and opened in June, is concealed from the main flow of patients, separating the offstage support areas from the onstage patient environment.

Credit: Assassi Productions/Courtesy of Taylor Design.
In addition to housing 17 medical and surgical specialties, the Scripps Clinic John R. Anderson V Medical Pavilion includes advanced cardiac catheterization labs for heart procedures, such as stents or pacemaker implants, in an outpatient setting.
Credit: HGA.
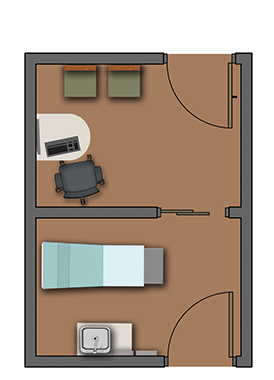
This diagram of a two-part exam room illustrates how a room might be divided into consult space and exam space.
Credit: HGA.
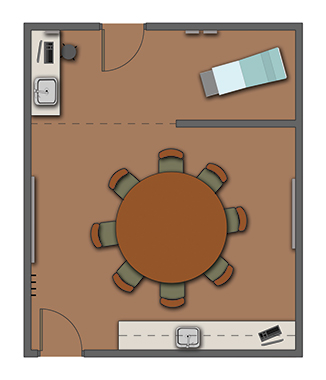
A group exam room diagram illustrates where multiple patients might meet for health education with an exam space at back.

Credit: Michael McLane Photography, Courtesy of Taylor Design.
This “corner office” space in the UCSF Medical Center Heart & Vascular Center in San Francisco, designed by Taylor Design, is set aside as a multipurpose, collaborative staff area.

Credit: Michael McLane Photography, Courtesy of Taylor Design.
An offstage hallway and shared work space in the staff hub of the UCSF Heart & Vascular Center allow direct access to patients via doors in the back of the exam rooms. The exam room also has a second door for patient use.

Credit:Michael McLane Photography, Courtesy of Taylor Design.
An offstage staff hub is just outside an exam room at the UCSF Heart & Vascular Center. The onstage/offstage design delineates between the public-facing spaces and staff and clinician-only spaces.
Need for clinic design is growing
It’s no secret that healthcare organizations across the country are shifting more and more services out of acute care settings. The move makes sense on a number of fronts, not least of which is the ability to reduce costs and improve outcomes all while increasing access and growing market share.
“The sheer volume of clinics being considered and built now is a stunning difference in the last five to 10 years,” says Ted Shaw, associate principal at Perkins+Will (New York).
The development of clinics—the catch-all term for pretty much any site that provides outpatient care, according to those who build them—is further inspired by healthcare reform pressing the need for population health management, with providers more invested than ever in keeping people well.
That mindset is requiring solutions like medical home models of care delivery and inspiring new builds and renovations that support collaborative, team-based environments, says Christine Guzzo Vickery, vice president at HGA Architects and Engineers (Minneapolis) and coauthor of Modern Clinic Design: Strategies for an Era of Change, published in 2015.
Although primary care is certainly a factor, Vickery says it’s mostly specialty and multispecialty practices behind the surge, including everything from women’s and children’s to sports medicine and orthopedic clinics. And colocating all providers involved in patients’ treatment plans under one roof goes a long way toward operational efficiency and, more important, patient satisfaction.
This current landscape is in large part the result of private physicians joining group practices at large healthcare systems and institutions creating specialty clinics to maximize their service offerings and broaden their reach. And exactly what shape those efforts take is key to providers differentiating themselves among the competition.
“The nature of the design environment is seen as just as important as bringing services to the community; it’s bringing it in the right package,” Shaw says.
Separating exam and consult space
Clinics are typically planned around 100- to 120-square-foot exam rooms—spaces large enough to accommodate more minimally invasive procedures than in the past, as well as family members accompanying patients on visits.
But what’s equally shaping projects is the consult room, as providers recognize that oftentimes clinic visits don’t require an exam at all. “The idea was [to shift] ‘from the exam table to the coffee table’—that was our mantra for what we were trying to do, to get patients to be more engaged in conversations with providers versus everything being about the exam,” says PJ Glasco, market sector leader and senior vice president at FKP (Houston), of the Children’s Hospital Colorado’s Multispecialty Clinic in Aurora, Colo., which was completed in May 2015.
To that end, the 22,000-square-foot shell build-out, which currently accommodates more than 40 clinics, includes 24 exam rooms and eight consult rooms, each split between two modules.
Similarly, Vickery says more and more providers are exploring separating the exam and consult space. “You walk in and you’re in the consult area, and then if you need to go have an exam, there’s a door to the exam area that’s in the back part of the room or in an adjacent room. That requires a larger exam room,” she says.
Also pushing square footage are group exam rooms often used for chronic illness management (diabetes, cardiac care) or OB/GYN services, Vickery says, with patients meeting collectively to discuss their conditions and receive health education while taking turns getting checkups in an adjacent exam space. It’s one solution answering the trend of more health and wellness education being offered in clinical settings, too.
“Even clinics that aren’t educational organizations themselves are often tied to academic medical centers. This has a direct effect on the design, because there’s a greater need for collaboration space and larger exam and meeting areas,” says Kevin Hinrichs, principal and director of Taylor Design’s San Francisco office.
(For more on clinic design, see coverage of an HCD Virtual educational session, “Searching For A Deeper Understanding Of Clinic Design.”)
Supporting staff in clinical spaces
For staff spaces, “clinic design today is moving away from dedicated physicians’ offices and offering more collaborative space for care team members,” says Randy Regier, president of Taylor Design (Irvine, Calif.). Onstage/offstage layouts are becoming increasingly popular to support that trend, with clinical staff housed in a central core, a solution Taylor Design used at the UCSF Medical Center Heart & Vascular Center in San Francisco, which opened in April.
The method supports collaborative care by creating group work areas where nurses and physicians work side by side, but also establishes an attractive buffer between patients and staff. “It’s quieter, more private, and it feels better to a patient,” Vickery says.
A consideration of the traditional onstage/offstage model is the space required to support separate corridors on each side of exam rooms for staff and patient circulation. After visiting a number of clinics with two-door models (separate staff and patient doors into exam rooms from those individual corridors), the project team at Scripps Clinic, John R. Anderson V Medical Pavilion in San Diego, which opened in June and was also designed by Taylor Design, opted for a variation.
“We’d have to sacrifice too many exam rooms and so much other space because of those common area hallways,” says Brett Ringler, senior director of clinic operations at Scripps Clinic (LaJolla, Calif.). The solution for that project is a single-door exam room with open care team stations located just outside the exam rooms.
“Onstage/offstage works well for a lot of things, but there are also other cases where they might have a teaming area that’s not offstage,” Vickery says. That’s the route taken at Children’s Hospital Colorado’s clinic, where the multidisciplinary staff collaborates in a central “fishbowl” where care teams work together but are readily available to patients and family members.
“We felt it was important for them to know where their providers were, so if they step out of the room they could easily see who was where,” says Janine Costantini, ambulatory practice director for Children’s Hospital Colorado. (Costantini and Glasco will share more about the Children’s Hospital Colorado project in the session “Meeting Complex Needs of Multispecialty Patients” [E75] at the 2016 Healthcare Design Expo & Conference.)
Planning for the future clinic
And as building uses are likely to change over time, designers are working to provide flexibility and adaptability throughout. Shaw recommends zoning spaces in the planning process, rather than fitting a program into the space without an overarching logic to it.
“If it’s purely that we’ve maximized every inch of it but we’ve put spaces in odd locations, then what happens in the future when you want to reallocate space? It becomes awkward and inflexible,” he says.
With the future in mind, many clinics are utilizing modular wall systems and common plumbing walls so a consult room can easily become an exam room or a team room might be converted to four exam rooms. “There’s a higher price tag to be paid for that initially, but I think it’s the way of the future,” Vickery says of modular solutions.
To stay nimble, providers are also requesting exam rooms that are as standardized as possible. At John R. Anderson V Medical Pavilion, 110 standardized exam rooms allow surgeons to practice in the same area as other physicians, and when they’re in surgery (40-60 percent of the time) those rooms don’t sit empty like they traditionally would. “Any doctor on any day can easily move from one set of exam rooms to the next, depending on volume,” Ringler says.
Patient experience drives clinic design
But if there’s any one driver inspiring clinic design today, it’s the patient experience. At Children’s Hospital Colorado, that came in realizing patients were traveling long distances to see multiple providers, often in disjointed visits throughout the course of a day—hours dictated by physicians’ schedules.
Instead, the hospital wanted to turn the tables. “It’s not that the patient is going to go see the provider, but the provider is now going to come see the patient,” Glasco says. “That was the germ of the idea for how to make it more patient-centric.”
It was a model the team didn’t quite find in a review of peer facilities across the country, with similar complex care clinics set up around a single provider as opposed to supporting multidisciplinary teams—so they created it.
The clinic hosts teams from various specialty clinics (e.g., ear, nose and throat; gastrointestinal; and endocrinology) who create multidisciplinary teams (e.g., treating cleft palate and spina bifida) to ensure that care team members are on hand to visit with patients and discuss treatment plans collectively.
Its 40-plus clinics then rotate days in the space, with most meeting once a month or every two weeks for two to eight hours, depending on the complexity of the disease. “That’s the biggest value of this is that it’s a shared space and utilized all the time,” Glasco says.
To design it, the team held a visioning session with about 50 stakeholders (including physicians, nurses, and IT and administrative staff) to establish guiding principles, figuring out how the space would look similar to traditional clinic models and where it might diverge, like the centralized “fishbowl” and larger exam rooms (140 square feet).
“It was truly a good collaboration between all the providers giving their thoughts on the difficulties they were facing and what might be solutions for how we’d resolve it,” Glasco says.
A similar approach was taken at the 175,000-square-foot John R. Anderson V Medical Pavilion, where Scripps was able to centralize its 12 outpatient cardiovascular specialties (from diabetes to pulmonary care) adjacent to its Prebys Cardiovascular Institute, with two bridges between the two buildings. The setting has allowed the provider to offer cardiac catheterizations in a less costly environment and include two general surgery suites and a c-arm-capable procedure room with a recovery bay, meaning physicians can easily balance their clinic practices with procedures simply by traveling between floors, or across the bridges to the hospital, if necessary.
The move frees up highly valuable time on the schedule so patients can be seen more quickly. “The idea is, if you give the doctors enough space, you can make the experience for the patient much more pleasant,” Ringler says.
Additional solutions for the patient experience include convenient parking, intuitive wayfinding, and a non-stressful and welcoming feel, Vickery says. “The patient journey is critical. Patients are demanding that, and providers are responding and understanding that if they’re not convenient, people aren’t going to come,” she says.
The overall feeling conveyed, Shaw adds, should be that the patient is taken care of, and designs should assuage feelings of anxiety with views outside or a glazed wall between waiting and clinical areas, for example. “These base, subliminal emotions are real for people, especially when in vulnerable places, and we need to do everything we can to create a complete antithesis of that,” he says.
How will telehealth change clinic spaces?
Just as hospitals brace for a future where only the highest acuity patients will likely be admitted as more care is delivered in outpatient settings, clinics will likely face a similar fate as more conditions are able to be managed right at home—a trend influencing the built environment in its own way. “People aren’t going to go to clinics as much; they’re not going to have to because they’re going to be able to email, FaceTime, or communicate in other ways without being present,” Vickery says.
For example, at Scripps, patients with automatic implantable cardioverter-defibrillators that require regular checkups can instead walk in front of a wand at home that “reads” the device and creates a digital file that’s sent to physicians remotely. “All those patients—into the hundreds in any given month—they don’t have to come in now and so you can more efficiently use the space,” Ringler says of the overall higher volume the provider is able to achieve thanks to the program.
At Children’s Hospital Colorado’s Multidisciplinary Clinic, telehealth has been beneficial for the provider with a seven-state reach to not always require patients to travel hours for a visit or to loop in a parent or primary care physician who can’t make the trip. “I feel this is a significant piece of where healthcare is going, because trying to get every provider who needs to be involved in a space at the same time is challenging. Telehealth will play a huge role for providers as well as families,” Costantini says.
To support efforts now, the clinic uses a conference room but is planning to add telehealth capability to exam rooms in the future, with modular wall systems allowing the ability to take out a panel and replace it with a monitor. “It goes to the point of showing you can add monitors and connectivity to the exam room without a whole lot of construction,” Glasco says.
Vickery anticipates technology even further influencing clinic operations, too, by streamlining workflow and care delivery, requiring designers to create flexible space that’s able to adapt as technology evolves. “[Clinics] will be much more high-tech when you get in there. You will be taking yourself to the exam room, you will check in online, schedule your appointment online. There will be a lot more happening electronically and virtually. It’s very exciting to think about how efficient we can make this,” she says.
Jennifer Kovacs Silvis is executive editor of Healthcare Design. She can be reached at jennifer.silvis@emeraldexpo.com.


